Imaging Case 10:
Prostate cancer – Adenocarcinoma
Nerve-sparing radical prostatectomy aims to reduce postoperative impotence, but this comes at the cost of a higher probability of incomplete resection. In this case, we illustrate how intraoperative specimen PET-CT imaging with 18F-PSMA can visualize the tumor in the resected tissue specimen. This could aid the surgeon in deciding whether it is necessary to remove more tissue intraoperatively.
This clinical case is courtesy of PD Dr. C. Darr and Prof. B. Hadaschik, Department of Urology, Universitätsmedizin Essen and is part of a case series published in European Urology Open Science in 2023.
Patient History
A patient diagnosed with an anterior high-risk prostate cancer (Gleason score 9) underwent bilateral nerve-sparing radical robot-assisted prostatectomy, followed by excision of the pelvic lymph nodes. The patient was injected with 268 MBq 18F-labelled prostate specific membrane antigen (18F-PSMA) on the morning of surgery. After exclusion of metastases by PSMA-PET/CT, surgery was performed on the same day.
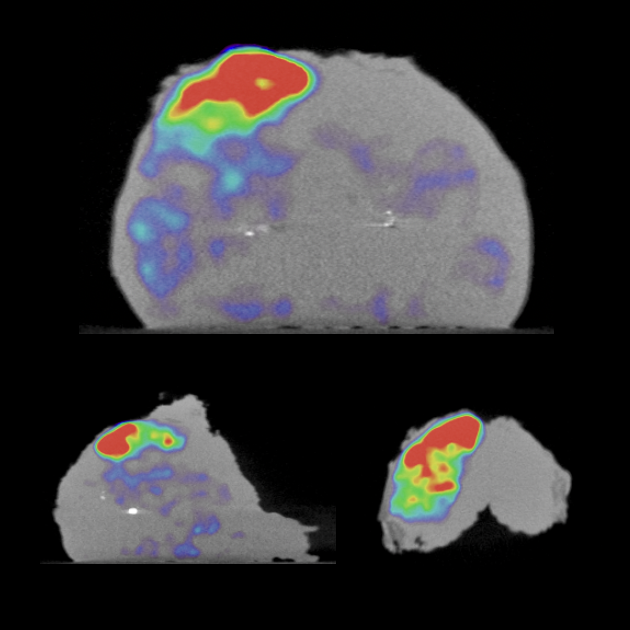
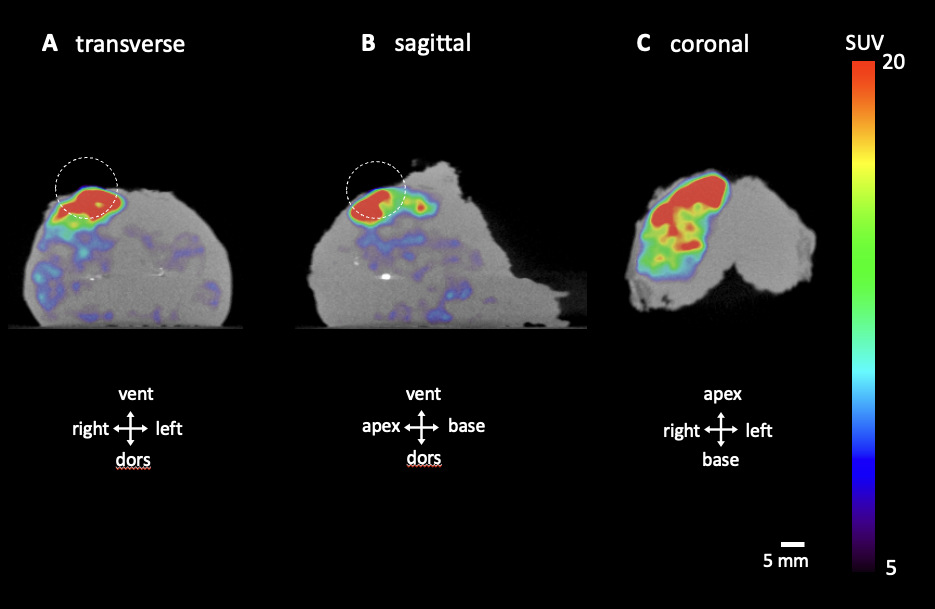 Figure 1. Transverse (A), sagittal (B) and coronal (C) slices of the specimen PET-CT images. The tumor is represented by a bright colorful region in the specimen. Surgical orientation of the specimen images is shown in each image. The PET tracer scale bar is depicted on the right hand side. The ellipse highlights a region of radiotracer uptake reaching the border of the specimen.
Figure 1. Transverse (A), sagittal (B) and coronal (C) slices of the specimen PET-CT images. The tumor is represented by a bright colorful region in the specimen. Surgical orientation of the specimen images is shown in each image. The PET tracer scale bar is depicted on the right hand side. The ellipse highlights a region of radiotracer uptake reaching the border of the specimen.
PET-CT specimen images
Once the prostate specimen was resected, it was immediately imaged inside the operating room with the XEOS AURA 10 PET-CT specimen imager. This was approximately 5 hours after injection of the radiotracer. Two orthogonal views of the specimen PET-CT images are depicted in Figure 1. The PET images are represented in color scale, superimposed on the CT images in greyscale.
The tumor is visualized inside the specimen as the bright colored region. At the right ventral side of the specimen, 18F-PSMA uptake is seen that reaches the border of the specimen. Tumor localization is far away from the dorsolateral neurovascular bundles. Within this feasibility study surgery was not adapted based on intraoperative imaging.
Findings and diagnosis
After finalization of surgery, the resected tumor was sent to the pathology department for histopathological examination. The histopathological results are listed in Table 1, and demonstrate a positive surgical margin at the right ventral border of the specimen.

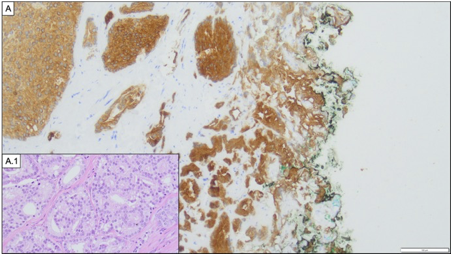 Figure 2. Histopathological image of the cancer and positive surgical margin. (A) Histopathological positive surgical margin R1 (2.5 mm, ventral right; 100x) with a Gleason grade 4 pattern. For better illustration, a pan-cytokeratin immunostain is shown. (A.1) A detailed microphotograph of the cancer (200x) is shown in hematoxylin and eosin staining exhibiting Gleason grade 4 pattern architecture. Reproduced from Darr C. et al. European Urology Open Science 54:28-32.
Figure 2. Histopathological image of the cancer and positive surgical margin. (A) Histopathological positive surgical margin R1 (2.5 mm, ventral right; 100x) with a Gleason grade 4 pattern. For better illustration, a pan-cytokeratin immunostain is shown. (A.1) A detailed microphotograph of the cancer (200x) is shown in hematoxylin and eosin staining exhibiting Gleason grade 4 pattern architecture. Reproduced from Darr C. et al. European Urology Open Science 54:28-32.
Discussion and conclusion
The specimen PET-CT images show a promising correlation with histopathology. The images specifically highlight radiotracer uptake at the right ventral border of the specimen where histopathological analysis finds a positive surgical margin. Availability of this information at the point of surgery could possibly help the surgeon enhance surgical outcomes.
REFERENCES
Darr C et al. (2023). Intraoperative Molecular Positron Emission Tomography Imaging for Intraoperative Assessment of Radical Prostatectomy Specimens. European Urology Open Science 54:28-32