Imaging Case 11:
Prostate cancer – Adenocarcinoma
Radical prostatectomy is the surgical treatment of choice in high-risk prostate cancer. Unfortunately, surgery in high-risk prostate cancer is associated with a considerable rate of positive surgical margins, which is in turn a risk factor for recurrence. Pelvic lymph node dissection is also performed during prostate cancer surgery, with the aim of obtaining detailed prognostic information as well as removing metastatically invaded lymph nodes detected on preoperative imaging. However, removal of all suspicious lymph nodes during surgery can be challenging. For both issues, the surgeon lacks information during surgery to enable well-informed decisions.
This clinical case illustrates how the information that is provided by performing intraoperative specimen PET-CT imaging with PSMA-PET can help the surgeon enhance surgical outcomes by providing a clear view of what was resected – right at the point of surgery. The case is courtesy of Prof. F. Ceci and colleagues, Department of Nuclear Medicine, European Institute of Oncology (Milan, Italy) and is part of a case series published in Biomedicines in 2023.
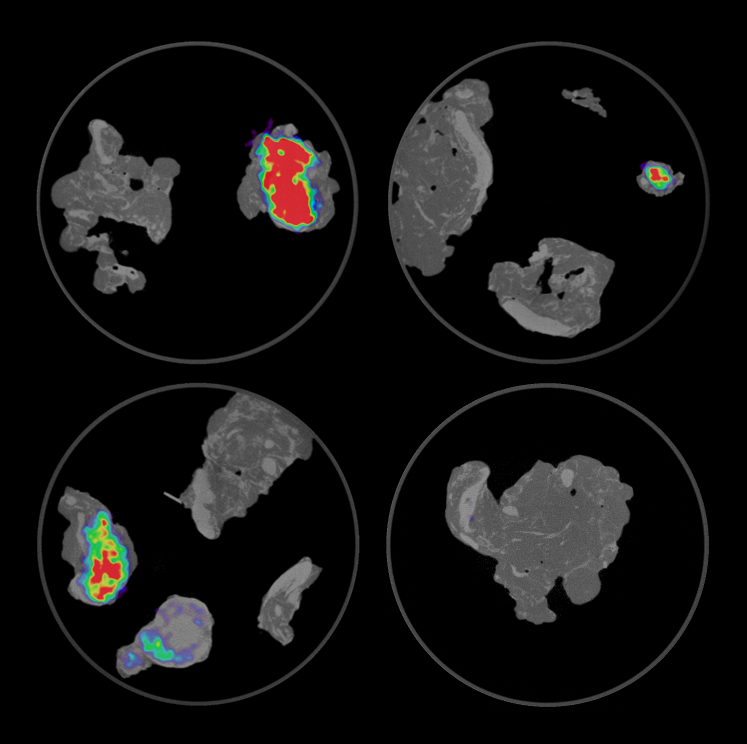
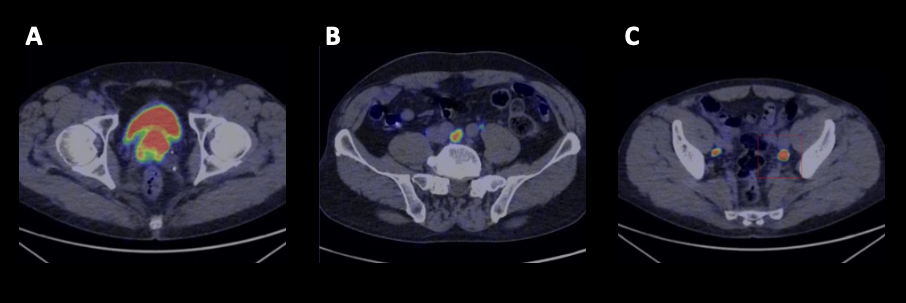 Figure 1. Transverse slices of the whole-body 68Ga-PSMA-PET-CT images acquired 4-6 weeks before surgery. High uptake is shown in the prostate gland (A) as well as in several lymph nodes (B, C).
Figure 1. Transverse slices of the whole-body 68Ga-PSMA-PET-CT images acquired 4-6 weeks before surgery. High uptake is shown in the prostate gland (A) as well as in several lymph nodes (B, C).
Patient History
A patient was diagnosed with high-risk prostatic adenocarcinoma (Gleason score 4+5). Whole-body PET imaging with 68Ga-PSMA was performed and demonstrated heterogeneous uptake in the entire prostate with suspicion of extracapsular extension. Additionally, PSMA-PET also showed two positive pelvic lymph nodes and one positive extrapelvic lymph node (Figure 1). The patient was considered miT3N1M1a based on the E-PSMA criteria.
The patient was scheduled for robot-assisted radical prostatectomy with pelvic lymph node dissection. To enable intraoperative specimen PET-CT imaging of the resected lesions, an injection of 1 MBq/kg (90 MBq) of 68Ga-PSMA was administered intravenously at the start of surgery.
PET-CT specimen images
Once the prostate specimen was resected, it was oriented in the specimen container and imaged inside the operating room with the XEOS AURA 10 PET-CT imager. Imaging of the main prostate specimen was done ca. 3.5 h after 68Ga-PSMA injection. Three orthogonal views of the specimen PET-CT images are depicted in Figure 2. The PET images are represented in color scale, superimposed on the CT images in greyscale.
The tumor is visualized inside the specimen as the bright colored region. At the left lateral and basal side of the specimen, 68Ga-PSMA uptake is seen that reaches the border.
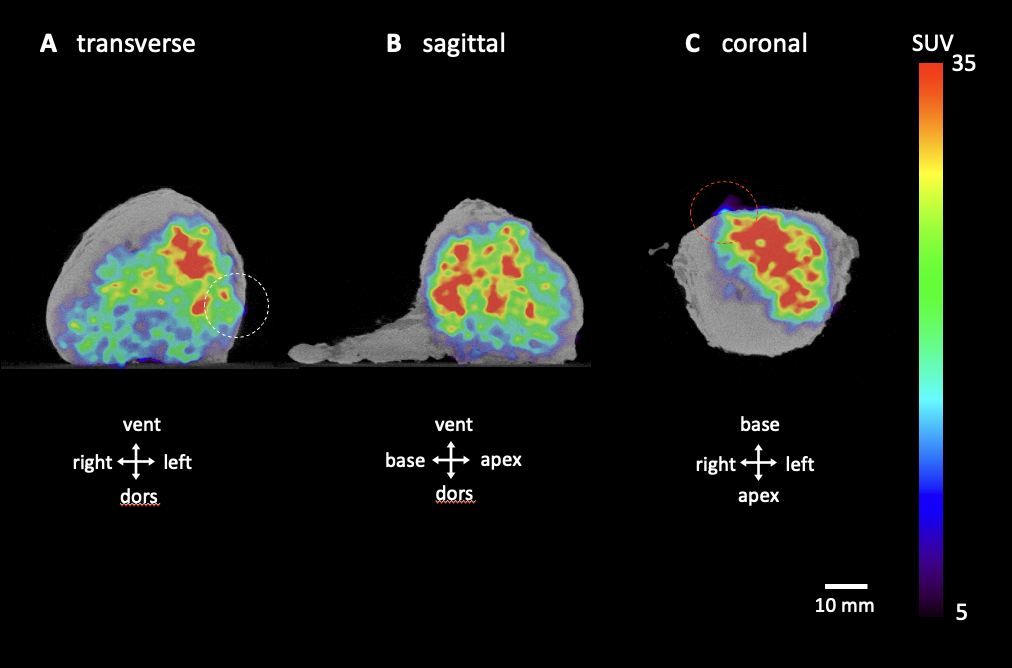 Figure 2. Transverse (A), sagittal (B) and coronal (C) slices of the specimen PET-CT images of the prostate specimen. The tumor is represented by a bright colorful region in the specimen. Surgical orientation of the specimen images is shown in each image. The PET tracer scale bar is depicted on the right hand side. The dashed circles highlight regions where the radiotracer uptake is reaching the left lateral (white) and basal (red) border of the specimen.
Figure 2. Transverse (A), sagittal (B) and coronal (C) slices of the specimen PET-CT images of the prostate specimen. The tumor is represented by a bright colorful region in the specimen. Surgical orientation of the specimen images is shown in each image. The PET tracer scale bar is depicted on the right hand side. The dashed circles highlight regions where the radiotracer uptake is reaching the left lateral (white) and basal (red) border of the specimen.
Subsequently, pelvic lymph node dissection was performed using a standard template. The resected lymph nodes were placed in specimen containers (4 in total) and also imaged using the XEOS AURA 10 PET-CT imager, approximately 4.5 h after radiotracer injection. Figure 3 shows specimen PET-CT images of the lymph nodes. Significant 68Ga-PSMA uptake is visualized in four lymph nodes, while other nodes do not show significant uptake.
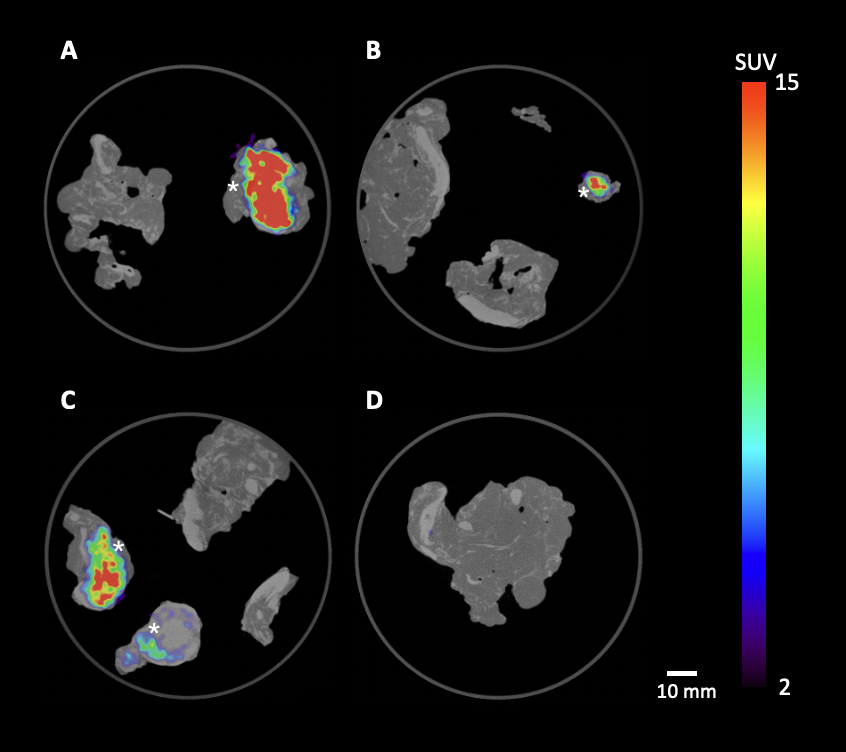 Figure 3. Specimen PET-CT images of resected pelvic and extrapelvic lymph nodes, distributed over 4 specimen containers (A-D). The PET tracer scale bar is depicted on the right hand side. The four lymph nodes marked with an asterisk (*) demonstrate significant 68Ga-PSMA uptake: left internal iliac (A), left peri-ureteral (B), right common iliac and obturator (C). The other lymph nodes did not show significant uptake.
Figure 3. Specimen PET-CT images of resected pelvic and extrapelvic lymph nodes, distributed over 4 specimen containers (A-D). The PET tracer scale bar is depicted on the right hand side. The four lymph nodes marked with an asterisk (*) demonstrate significant 68Ga-PSMA uptake: left internal iliac (A), left peri-ureteral (B), right common iliac and obturator (C). The other lymph nodes did not show significant uptake.
Findings and diagnosis
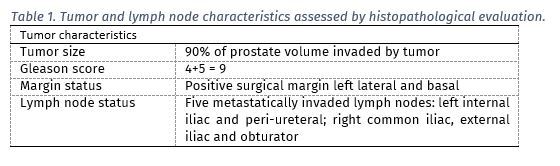
After finalization of surgery, the resected prostate specimen and lymph nodes were sent to the pathology department for histopathological examination. The histopathological results are listed in Table 1. A positive surgical margin was found at the left lateral and basal border of the prostate. This correlates with the region of high radiotracer uptake reaching the border of the specimen on the specimen PET-CT images. Metastatic invasion was detected in 5 lymph nodes. All lymph nodes that showed significant radiotracer uptake were also confirmed to be metastatically invaded.
Discussion and conclusion
The specimen PET-CT images showed an excellent correlation with histopathology. The images demonstrated 68Ga-PSMA uptake reaching the left lateral and basal border of the specimen, where histopathological analysis also detected a positive surgical margin. Good correlation was also found between the specimen PET-CT images of the lymph nodes and histopathology. Having this information available at the point of surgery could help guide surgical management and enhance outcomes.
REFERENCES
Muraglia L et al. (2023). First Live-Experience Session with PET/CT Specimen Imager: A Pilot Analysis in Prostate Cancer and Neuroendocrine Tumor. Biomedicines 11:645.