Imaging Case 13:
Angioblastic T-cell Lymphoma - Biopsy
18F-FDG PET-CT imaging is a common tool used to stage lymphoproliferative diseases. The final diagnosis is dependent on histopathological confirmation. Ideally, this confirmation should be obtained from the sites exhibiting the highest metabolic activity. Depending on the lymph node’s location, prelevation of the relevant tissue can be challenging. Depending on the location of the lymph node to be biopsied, it can be a challenge to obtain a representative sample. If postoperative analysis shows that the sample is not representative, the patient may need to undergo a second surgery to establish the diagnosis.
In this clinical case, we illustrate how specimen PET-CT imaging can be used to ensure that a representative biopsy is obtained. The case is presented with the support of dr. Valérie Vergucht and prof. dr. Bieke Lambert of AZ Maria Middelares, Ghent, Belgium.
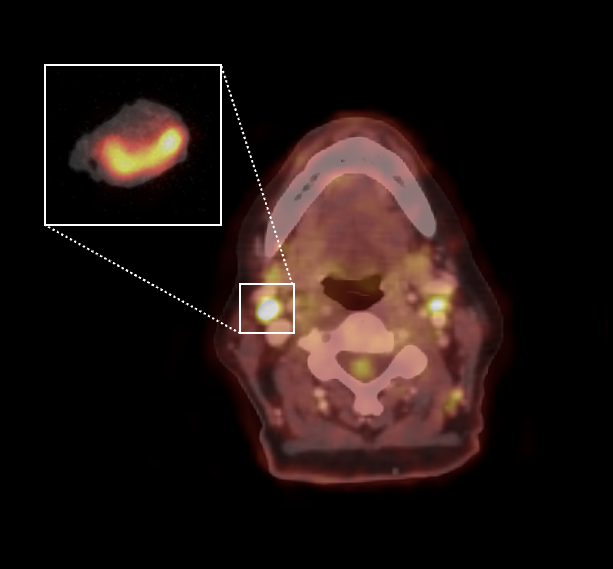
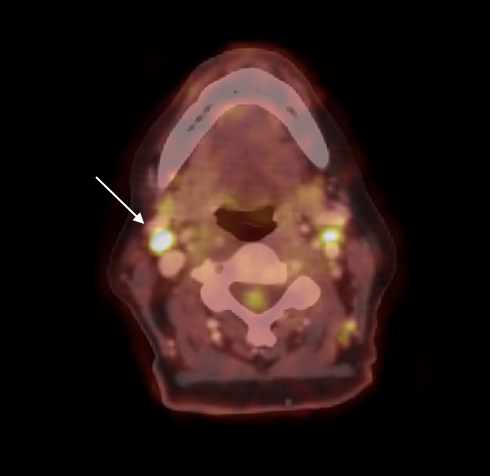 Figure 1: Selection of a metabolically active lymph node in the right cervical region 2A (white arrow) with SUVmax 13.5 and SUVmean 7.1; the longest axis of the node was 14mm.
Figure 1: Selection of a metabolically active lymph node in the right cervical region 2A (white arrow) with SUVmax 13.5 and SUVmean 7.1; the longest axis of the node was 14mm.
Patient History
A 73-year-old woman presented with clinically enlarged lymph nodes and splenomegaly. A 18F-FDG PET-CT scan revealed multiple lymph nodes on both sides of the diaphragm with highly increased tracer uptake. An axillary lymph node was resected in an attempt to diagnose lymphoma. However, this lymph node only yielded reactive lymphoid tissue, with no evidence of malignancy. Consequently, a second surgery was scheduled to resect a supraclavicular lymph node. The diagnosis of angioblastic T cell lymphoma was established. Systemic CHOP chemotherapy was prescribed and interim whole body 18F-FDG PET- CT scan showed a complete metabolic response 3 months later.
PET-CT specimen images
The patient was injected with 4 MBq/kg 18F-FDG at the nuclear medicine department approximately 1 hour before the start of surgery. Resection of the lymph node was completed at approximately 1.5 h after injection. Immediately after resection, a 10 minute high-resolution specimen PET-CT image was acquired in the operating theatre. The images are shown in fig. 2.
The images of the lymph node clearly show increased 18F-FDG uptake with SUVmax of 9.44. The image was interpreted during surgery in the operating theatre to help confirm that the target lymph node was resected.
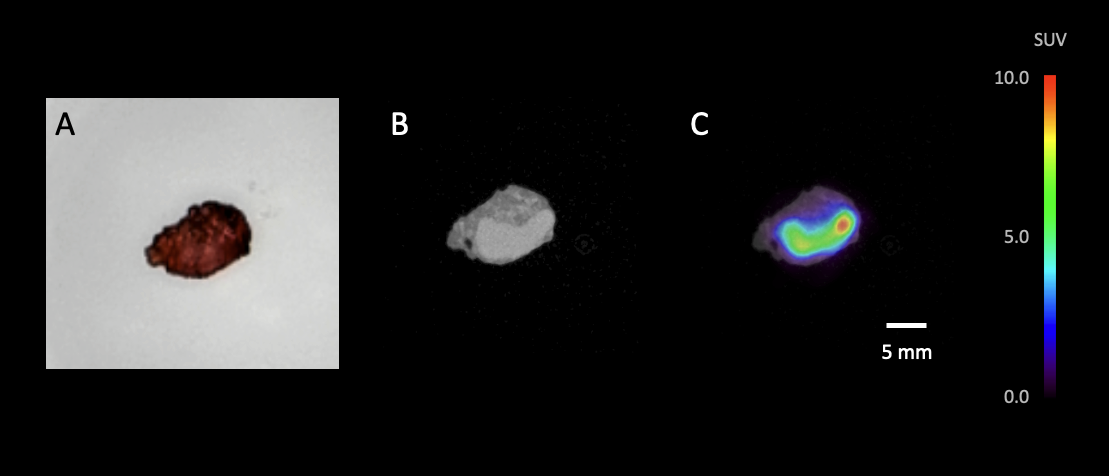 Figure 2. High-resolution specimen PET-CT images of the resected lymph node sample, as shown to the surgeon in the operating theatre. (A) optical image of the resected lymph node placed in the specimen container; (B) representative slice of the CT image; (C) representative slice of the PET-CT image, showing an SUVmax of 9.44.
Figure 2. High-resolution specimen PET-CT images of the resected lymph node sample, as shown to the surgeon in the operating theatre. (A) optical image of the resected lymph node placed in the specimen container; (B) representative slice of the CT image; (C) representative slice of the PET-CT image, showing an SUVmax of 9.44.
Histopathological Evaluation
After specimen imaging, the resected specimen was sent to the pathology department for routine histopathological evaluation, which was available after several days. Immuno-histopathology confirmed persistent angioblastic T cell lymphoma. Hence, the end-of-treatment 18F-FDG PET-CT and histopathological findings were considered as confirmed progression of disease despite the earlier complete remission.
Discussion and conclusion
This case demonstrates the utility of specimen PET-CT imaging in providing surgeons with the immediate assurance that the lymph node most pertinent for histopathological evaluation has been successfully resected.
The initial diagnosis of the patient was postponed due to a negative histopathology result, since the first biopsy involved the resection of an unaffected lymph node. However, when the follow-up 18F-FDG PET-CT revealed recurrence of suspicious metabolic activity in multiple lymph nodes, despite the absence of palpable disease, we effectively utilized intraoperative specimen PET-CT imaging to prevent futile biospy. The surgeon correctly removed the FDG-avid lymph node, which was confirmed by the use of the AURA high resolution PET-CT specimen scan within 10 minutes. Final histopathology confimed the recurrence of the angioblastic T-cell lymphoma.