Imaging Case 5:
Prostate Cancer - Adenocarcinoma
Radical prostatectomy often requires sacrificing the neurovascular bundle, which impacts the quality of life of prostate cancer patients. A nerve-sparing approach can be used, but this involves an increased risk of incomplete resection. Therefore, it is interesting to know intraoperatively whether the tumor has been sufficiently removed when performing nerve-sparing surgery.
Prostate cancer cells have an increased PSMA expression, which is how they can be distinguished from healthy prostatic tissue on whole-body PSMA PET-CT [1]. In this clinical case, we highlight how intraoperative specimen PSMA PET-CT imaging visualizes the tumor within the specimen. This could aid the surgeon in deciding whether it is necessary to remove more tissue intraoperatively when aiming for a complete resection.
This clinical case is courtesy of Dr. C. Darr and Prof. B. Hadaschik, Department of Urology, Universitätsmedizin Essen.
Patient history
A patient diagnosed with high-risk prostatic adenocarcinoma (Gleason score 9) underwent radical robot-assisted prostatectomy, followed by excision of the pelvic lymph nodes. The patient was injected with 167MBq 68Ga-labelled prostate specific membrane antigen (68Ga-PSMA) on the morning of surgery. After exclusion of metastases by PSMA-PET/CT, surgery was performed on the same day.
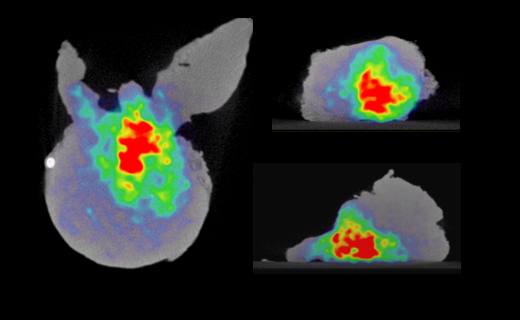
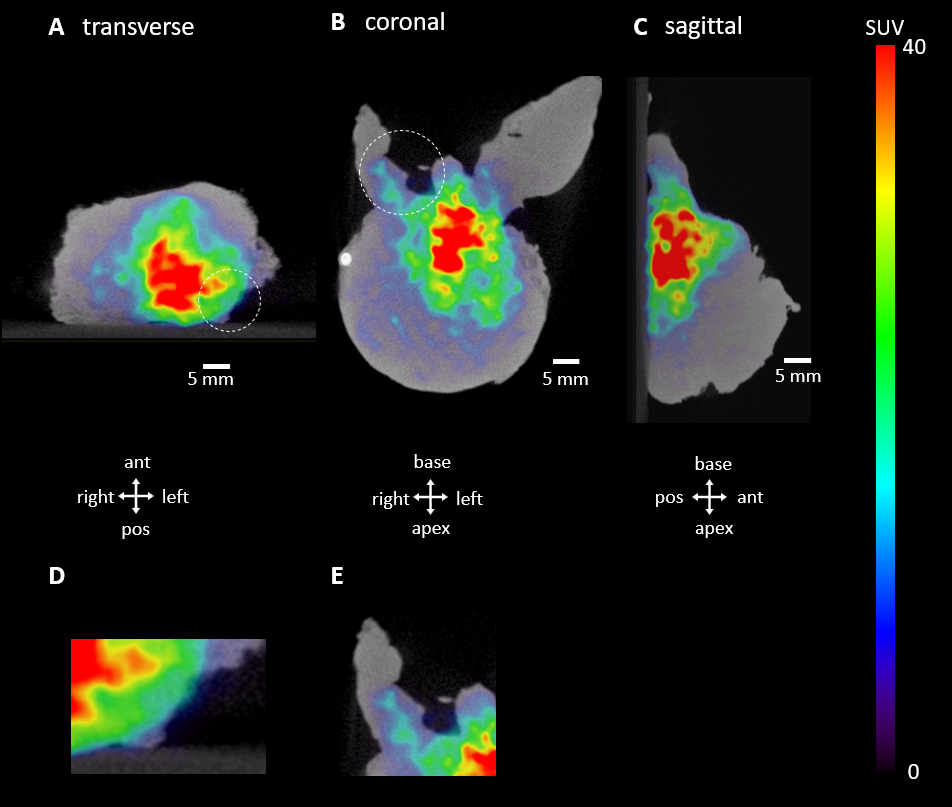 Figure 1. Transverse (A), coronal (B) and sagittal (C) slides of the specimen PET-CT images. The tumor is represented by a bright colorful region in the specimen. Surgical orientation of the specimen images is shown at the bottom of each section. The PET tracer scale bar is depicted on the right hand side. Abbreviations: ant, anterior; pos, posterior. D) Detail of radiotracer uptake near the left posterior border. E) Detail of radiotracer uptake in the right seminal vesicle and vas deferens.
Figure 1. Transverse (A), coronal (B) and sagittal (C) slides of the specimen PET-CT images. The tumor is represented by a bright colorful region in the specimen. Surgical orientation of the specimen images is shown at the bottom of each section. The PET tracer scale bar is depicted on the right hand side. Abbreviations: ant, anterior; pos, posterior. D) Detail of radiotracer uptake near the left posterior border. E) Detail of radiotracer uptake in the right seminal vesicle and vas deferens.
PET-CT specimen images
At the left posterior border of the specimen image, increased 68Ga-PSMA uptake can be seen. There is also increased uptake in the right seminal vesicle.
The CT images reveal the anatomy of the specimen. Figure 2 depicts a coronal section of the CT scan. The seminal vesicles and left and right vas deferens are clearly visible at the base of the prostate. In combination with the information provided by the PET images this may give more insight into what extent the tumor is present in the specimen.
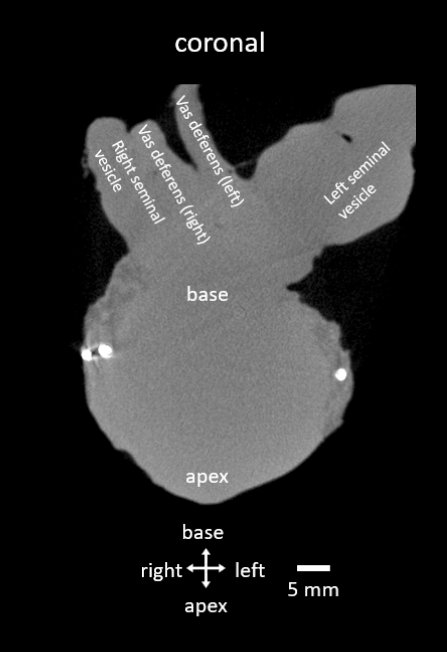 Figure 2. Coronal view of the CT scan of the resected prostate specimen. Anatomical structure of the specimen is indicated.
Figure 2. Coronal view of the CT scan of the resected prostate specimen. Anatomical structure of the specimen is indicated.
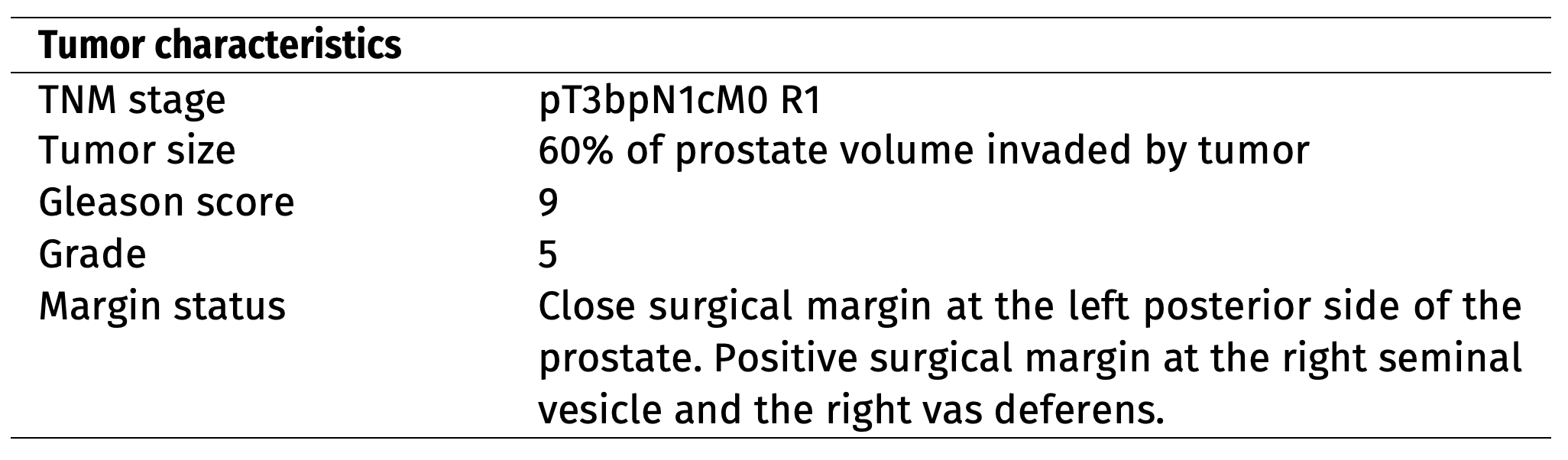 Table 1. Tumor characteristics assessed by histopathological evaluation.
Table 1. Tumor characteristics assessed by histopathological evaluation.
Findings and diagnosis
After specimen PET-CT imaging, the resected tumor was sent to the pathology department for histopathological examination. The histopathological results are listed in Table 1.
Discussion and conclusion
The PET-CT images indicate radiotracer uptake reaching the left posterior border of the resected specimen, which can be correlated to a close resection margin on histopathological analysis. 68Ga-PSMA uptake is also visible in the right seminal vesicle and right vas deferens, which can be correlated to tumoral invasion of both structures on histopathological analysis.REFERENCES
[1] Okarvi, S. M. Recent developments of prostate-specific membrane antigen (PSMA)-specific radiopharmaceuticals for precise imaging and therapy of prostate cancer: an overview. Clin. Transl. Imaging 7, 189–208. issn: 22817565 (June 2019).